Zamówienia złożone w dniach 29.04 - 06.05 zostaną wysłane po 06.05. Aby zrekompensować te niedogodności, zamówienia złożone w tym terminie są objęte Majówkową Darmową Dostawą >
Podsumowanie
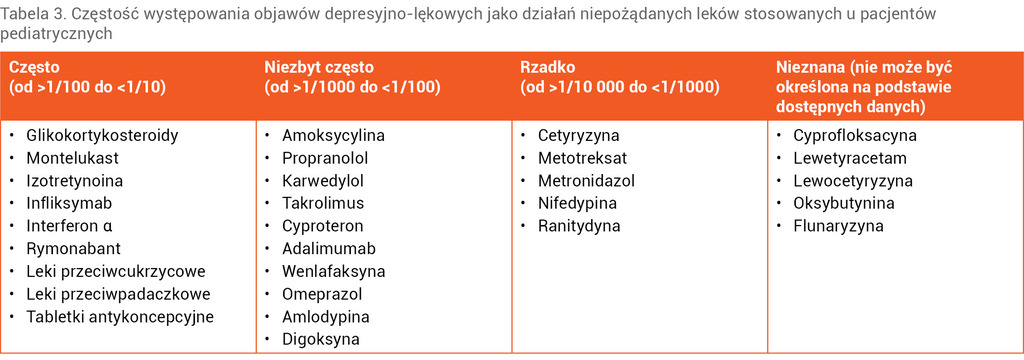
Tabela 3. Częstość występowania objawów depresyjno-lękowych jako działań niepożądanych leków stosowanych u pacjentów pediatrycznych
Wiedza dotycząca skutków ubocznych farmakoterapii w populacji pacjentów pediatrycznych (tab. 3), w tym uważność w zakresie objawów związanych z zaburzeniami psychicznymi, ma bardzo duże znaczenie w procesie leczenia małoletniego pacjenta. Działania niepożądane leków u dzieci są częste, mogą nieść ze sobą negatywne skutki nie tylko somatyczne, lecz także w sferze psychicznej, a tym samym mieć znaczący wpływ na powodzenie leczenia oraz jakość życia pacjentów. Zaburzenia psychiczne były czwartą po zaburzeniach ogólnych, zaburzeniach skóry i tkanki podskórnej oraz zaburzeniach układu nerwowego najczęściej zgłaszaną grupą objawów. Zazwyczaj występujące zaburzenia związane są z zaburzeniami depresyjnymi i lękowymi, a im wcześniejszy wiek zachorowania u dziecka, tym bardziej prawdopodobne są trudności społeczne i zawodowe, gorsza jakość życia oraz większe problemy ze zdrowiem fizycznym i psychicznym, więcej epizodów depresji w ciągu życia i więcej prób samobójczych23. Szacuje się, że depresja powoduje większą niepełnosprawność u ludzi w wieku 10-24 lat niż jakakolwiek inna choroba26. Podobne dane kształtują się w odniesieniu do zaburzeń lękowych, które są wyniszczające i często powodują upośledzenie funkcjonowania społecznego i zawodowego pacjenta27,28. Ważny jest wgląd w występowanie i charakter psychiatrycznych powikłań stosowania farmakoterapii w populacji dziecięcej. Może to pomóc pediatrom w przewidywaniu i rozpoznawaniu tych reakcji, a co za tym idzie, we wdrożeniu efektywnych oddziaływań.
ABSTRACT
Anxiety and depressive disorders – what every pediatrician should look out for
One in four people will experience a mental disorder in adulthood, and around one in five people will experience a mental disorder at some point in childhood and adolescence. Most cases of mental disorders are actually believed to derive from early childhood or adolescence, causing a significant burden in later life. Half of all cases of psychopathology in one’s lifetime manifest most often at the age of 14. The prevalence of anxiety and depressive disorders is estimated at 5%-7% and 2%, respectively, at the age of 9-11 years, with some indications that the prevalence of anxiety may be even higher. These rates increase to 32% and 14%, respectively, during puberty. With regard to depressive and anxiety disorders in underage patients, it is particularly worth paying attention to the pharmacotherapy used in this group, which is related to the occurrence of this type of disorder. Adverse drug reactions (ADR) in pediatric patients are frequent; apart from somatic negative effects, they can produce negative effects also in the mental sphere and thus have a significant impact on the success of treatment and the quality of life of patients.
Piśmiennictwo
1. Georgiades K, Duncan L, Wang L, et al.; 2014 Ontario Child Health Study Team. Six-month prevalence of mental disorders and service contacts among children and youth in Ontario: evidence from the 2014 Ontario Child Health Study. Can J Psychiatry 2019;64(4):246-55
2. Westerhof GJ, Keyes CL. Mental illness and mental health: the two continua model across the lifespan. J Adult Dev 2010;17(2):110-9
3. Waddell C, Schwartz C, Andres C. Making children’s mental health a public policy priority: for the one and the many. Public Health Ethics 2018;11:191-200
4. Kessler RC, Berglund P, Demler O, et al. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry 2005;62(6):593-602
5. Copeland WE, Angold A, Shanahan L, et al. Longitudinal patterns of anxiety from childhood to adulthood: the Great Smoky Mountains Study. J Am Acad Child Adolesc Psychiatry 2014;53(1):21-33
6. Ghandour RM, Sherman LJ, Vladutiu CJ, et al. Prevalence and treatment of depression, anxiety and conduct problems in US children. J Pediatr 2019;206:256-67
7. Cartwright-Hatton S, McNicol K, Doubleday E. Anxiety in a neglected population: prevalence of anxiety disorders in pre-adolescent children. Clin Psychol Rev 2006;26(7):817-33
8. Merikangas KR, He JP, Burstein M, et al. Service utilization for lifetime mental disorders in U.S. adolescents: results of the National Comorbidity Survey-Adolescent Supplement (NCS-A). J Am Acad Child Adolesc Psychiatry 2011;50(1):32-45
9. Al-Yagon M. Maternal emotional resources and socio-emotional well-being of children with and without learning disabilities. Family Relations 2010;59(2):152-69
10. Bonifacci P, Storti M, Tobia V, et al. Specific learning disorders: a look inside children's and parents' psychological well-being and relationships. J Learn Disabil 2016;49(5):532-45
11. Nosarti C, Reichenberg A, Murray RM, et al. Preterm birth and psychiatric disorders in young adult life. Arch Gen Psychiatry 2012;69(6):E1-8
12. Douglass LM, Heeren TC, Stafstrom CE, et al. Cumulative incidence of seizures and epilepsy in ten-year-old children born before 28 weeks' gestation. Pediatr Neurol 2017;73:13-9
13. Akshoomoff N, Joseph RM, Taylor HG, et al. Academic achievement deficits and their neuropsychological correlates in children born extremely preterm. J Dev Behav Pediatr 2017;38(8):627-37
14. Joseph RM, O'Shea TM, Allred EN, et al.; ELGAN Study Investigators. Neurocognitive and academic outcomes at age 10 years of extremely preterm newborns. Pediatrics 2016;137(4):e20154343
15. WHO. International Classification of Diseases 11th Revision. Geneva: World Health Organization, 2019
16. APA. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington: American Psychiatric Association, 2013
17. DC:0-5™: Diagnostic classification of mental health and developmental disorders of infancy and early childhood. Washington: Zero to Three, 2016
18. Popek L, Remberk B. Zaburzenia depresyjne u dzieci i młodzieży. W: Janas-Kozik M, Wolańczyk T (red.). Psychiatria dzieci i młodzieży. Tom 1. Warszawa: Wydawnictwo Lekarskie PZWL, 2021:472-93
19. Thapar A, Collishaw S, Pine DS, et al. Depression in adolescence. Lancet 2012;379(9820):1056-67
20. Maughan B, Collishaw S, Stringaris A. Depression in childhood and adolescence. J Can Acad Child Adolesc Psychiatry 2013;22(1):35-40
21. Hyde JS, Mezulis AH, Abramson LY. The ABCs of depression: integrating affective, biological and cognitive models to explain the emergence of the gender difference in depression. Psychol Rev 2008;115(2):291-313
22. Fergusson DM, Boden JM, Horwood LJ. Recurrence of major depression in adolescence and early adulthood, and later mental health, educational and economic outcomes. Br J Psychiatry 2007;191:335-42
23. Zisook S, Lesser I, Stewart JW, et al. Effect of age at onset on the course of major depressive disorder. Am J Psychiatry 2007;164(10):1539-46
24. Copeland WE, Wolke D, Shanahan L, et al. Adult functional outcomes of common childhood psychiatric problems: a prospective, longitudinal study. JAMA Psychiatry 2015;72(9): 892-9
25. Cash SJ, Bridge JA. Epidemiology of youth suicide and suicidal behavior. Curr Opin Pediatr 2009;21(5):613-9
26. Gore FM, Bloem PJ, Patton GC, et al. Global burden of disease in young people aged 10-24 years: a systematic analysis. Lancet 2011;377(9783):2093-102
27. Mendlowicz MV, Stein MB. Quality of life in individuals with anxiety disorders. Am J Psychiatry 2000;157(5):669-82
28. Stein MB, Roy-Byrne PP, Craske MG, et al. Functional impact and health utility of anxiety disorders in primary care outpatients. Med Care 2005;43(12):1164-70
29. Greenberg PE, Sisitsky T, Kessler RC, et al. The economic burden of anxiety disorders in the 1990s. J Clin Psychiatry 1999;60(7):427-35
30. Andlin-Sobocki P, Jönsson B, Wittchen HU, et al. Cost of disorders of the brain in Europe. Eur J Neurol 2005;12(Suppl 1):1-27
31. Bittner A, Egger HL, Erkanli A, et al. What do childhood anxiety disorders predict? J Child Psychol Psychiatry 2007;48(12):1174-83
32. Benjamin CL, Harrison JP, Settipani CA, et al. Anxiety and related outcomes in young adults 7 to 19 years after receiving treatment for child anxiety. J Consult Clin Psychol 2013;81(5):865-76
33. Anholt GE, Aderka IM, van Balkom AJ, et al. Age of onset in obsessive-compulsive disorder: admixture analysis with a large sample. Psychol Med 2014;44(1):185-94
34. Lim SW, Ha J, Shin YC, et al. Clinical differences between early- and late-onset social anxiety disorders. Early Interv Psychiatry 2013;7(1):44-50
35. Pilecki M, Łucka I. Zaburzenia lękowe. W: Janas-Kozik M, Wolańczyk T (red.). Psychiatria dzieci i młodzieży. Tom 1. Warszawa: Wydawnictwo Lekarskie PZWL, 2021:545-89
36. Stein MB. An epidemiologic perspective on social anxiety disorder. J Clin Psychiatry 2006;67(Suppl 12):3-8
37. Burstein M, He JP, Kattan G, et al. Social phobia and subtypes in the national comorbidity survey-adolescent supplement: prevalence, correlates and comorbidity. J Am Acad Child Adolesc Psychiatry 2011;50(9):870-80
38. Aderka IM, Hofmann SG, Nickerson A, et al. Functional impairment in social anxiety disorder. J Anxiety Disord 2012;26(3):393-400
39. Ruscio AM, Brown TA, Chiu WT, et al. Social fears and social phobia in the USA: results from the National Comorbidity Survey Replication. Psychol Med 2008;38(1):15-28
40. Leyfer O, Gallo KP, Cooper-Vince C, et al. Patterns and predictors of comorbidity of DSM-IV anxiety disorders in a clinical sample of children and adolescents. J Anxiety Disord 2013;27(3):306-11
41. Buckner JD, Schmidt NB, Lang AR, et al. Specificity of social anxiety disorder as a risk factor for alcohol and cannabis dependence. J Psychiatr Res 2008;42(3):230-9
42. Hofflich SA, Hughes AA, Kendall PC. Somatic complaints and childhood anxiety disorders. Int J Clin Health Psychol 2006;6:229-42
43. Crawley SA, Caporino NE, Birmaher B, et al. Somatic complaints in anxious youth. Child Psychiatry Hum Dev 2014;45(4):398-407
44. May AC, Rudy BM, Davis TE 3rd, et al. Somatic symptoms in those with performance and interaction anxiety. J Health Psychol 2014;19(11):1400-9
45. Ginsburg GS, Riddle MA, Davies M. Somatic symptoms in children and adolescents with anxiety disorders. J Am Acad Child Adolesc Psychiatry 2006;45(10):1179-87
46. Ramsawh HJ, Chavira DA, Stein MB. Burden of anxiety disorders in pediatric medical settings: prevalence, phenomenology and a research agenda. Arch Pediatr Adolesc Med 2010;164(10):965-72
47. Masia Warner C, Reigada LC, Fisher PH, et al. CBT for anxiety and associated somatic complaints in pediatric medical settings: an open pilot study. J Clin Psychol Med Settings 2009;16(2):169-77
48. Clavenna A, Bonati M. Adverse drug reactions in childhood: a review of prospective studies and safety alerts. Arch Dis Child 2009;94(9):724-8
49. Ekhart C, Vries T, Hunsel FV. Psychiatric adverse drug reactions in the paediatric population. Arch Dis Child 2020;105(8):749-55
50. Hales CM, Kit BK, Gu Q, et al. Trends in prescription medication use among children and adolescents – United States, 1999-2014. JAMA 2018;319(19):2009-20
51. Aagaard L, Weber CB, Hansen EH. Adverse drug reactions in the paediatric population in Denmark: a retrospective analysis of reports made to the Danish Medicines Agency from 1998 to 2007. Drug Saf 2010;33(4):327-39
52. Brown ES, Khan DA, Nejtek VA. The psychiatric side effects of corticosteroids. Ann Allergy Asthma Immunol 1999;83(6 Pt 1):495-503
53. Warrington TP, Bostwick JM. Psychiatric adverse effects of corticosteroids. Mayo Clin Proc 2006;81(10):1361-7
54. Stuart FA, Segal TY, Keady S. Adverse psychological effects of corticosteroids in children and adolescents. Arch Dis Child 2005;90(5):500-6
55. Bender BG, Lerner JA, Kollasch E. Mood and memory changes in asthmatic children receiving corticosteroids. J Am Acad Child Adolesc Psychiatry 1988;27(6):720-5
56. Aldea Perona A, García-Sáiz M, Sanz Álvarez E. Psychiatric disorders and montelukast in children: a disproportionality analysis of the VigiBase(®). Drug Saf 2016;39(1):69-78
57. Karakuła-Juchnowicz H, Kowal-Popczak A, Stelmach E i wsp. Przeciwdepresyjne czy depresjogenne efekty leczenia trądziku izotretynoiną? Dermatol Klin 2014;16(2):76-82
58. Saadoun D, Resche Rigon M, Thibault V, et al. Peg-IFNα/ribavirin/protease inhibitor combination in hepatitis C virus associated mixed cryoglobulinemia vasculitis: results at week 24. Ann Rheum Dis 2014;73(5):831-7
59. González-Peralta RP, Kelly DA, Haber B, et al.; International Pediatric Hepatitis C Therapy Group. Interferon alfa-2b in combination with ribavirin for the treatment of chronic hepatitis C in children: efficacy, safety and pharmacokinetics. Hepatology 2005;42(5):1010-8
60. Sherman KE. Managing adverse effects and complications in completing treatment for hepatitis C virus infection. Top Antivir Med 2012;20(4):125-8
61. Shayowitz M, Bressler M, Ricardo AP, et al. Infliximab-induced depression and suicidal behavior in adolescent with Crohn's disease: case report and review of literature. Pediatr Qual Saf 2019;4(6):e229
62. Moreira FA, Crippa JA. The psychiatric side-effects of rimonabant. Braz J Psychiatry 2009;31(2):145-53
63. Berge LI, Riise T, Fasmer OB, et al. Risk of depression in diabetes is highest for young persons using oral anti-diabetic agents. Diabet Med 2012;29(4):509-14
64. Reynolds KA, Helgeson VS. Children with diabetes compared to peers: depressed? distressed? A meta-analytic review. Ann Behav Med 2011;42(1):29-41
65. Noh JH, Park JK, Lee HJ, et al. Depressive symptoms of type 2 diabetics treated with insulin compared to diabetics taking oral anti-diabetic drugs: a Korean study. Diabetes Res Clin Pract 2005;69(3):243-8
66. Patten SB, Love EJ. Drug-induced depression. Incidence, avoidance and management. Drug Saf 1994;10(3):203-19
67. Kemper MJ, Spartà G, Laube GF, et al. Neuropsychologic side-effects of tacrolimus in pediatric renal transplantation. Clin Transplant 2003;17(2):130-4
68. De Wit AE, Booij SH, Giltay EJ, et al. Association of use of oral contraceptives with depressive symptoms among adolescents and young women. JAMA Psychiatry 2020;77(1):52-9